First FDA Approval for HDV: A Milestone in Hepatology
The FDA approved Hepcludex (bulevirtide) as the first treatment for chronic HDV. Learn what this milestone means for patients with hepatitis delta.
Introduction
On May 22, 2026, the U.S. Food and Drug Administration (FDA) made history by approving Hepcludex (bulevirtide-gmod), the first and only treatment ever authorized for chronic hepatitis delta virus (HDV) infection. For patients who have lived with a disease once called "the most severe form of viral hepatitis," this approval ends decades of empty-handed clinic visits.
HDV infects an estimated 48 to 60 million people worldwide, yet until this approval, physicians had nothing specific to offer beyond general hepatitis B management. The gap in care was so profound that the FDA granted Hepcludex Breakthrough Therapy designation, Orphan Drug designation, and Priority Review before ultimately clearing it under the Accelerated Approval pathway.
This article explains what HDV is, why it is uniquely dangerous, who qualifies for the new treatment, and what the evidence does and does not yet show. This article is for general informational purposes and does not replace the advice of a physician or hepatologist.
Causes and Symptoms
What Is HDV and How Does It Spread?
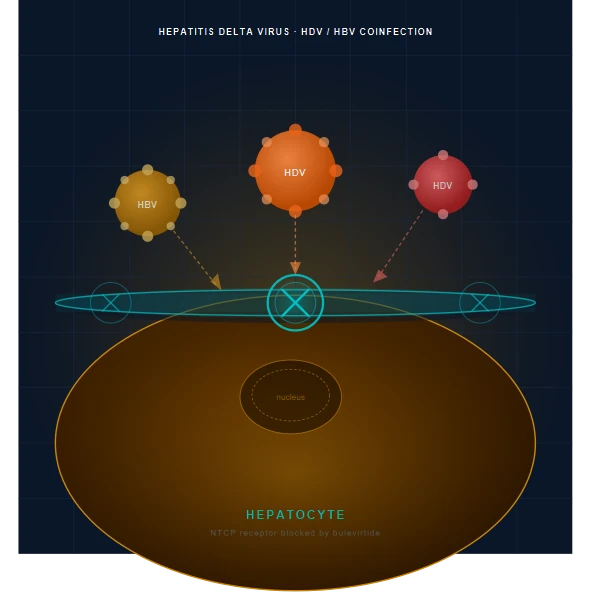
Hepatitis delta virus (HDV) is a small, defective single-stranded RNA virus that belongs to the genus Deltavirus. It is structurally unusual because it cannot infect liver cells independently: it requires the hepatitis B surface antigen (HBsAg), produced only by hepatitis B virus (HBV), to assemble new viral particles and enter hepatocytes.
This dependency means HDV infection can occur in two patterns
- Co-infection: a person acquires both HBV and HDV simultaneously, often leading to acute illness that resolves in most immunocompetent adults.
- Superinfection: a person with pre-existing chronic HBV acquires HDV on top of it. Superinfection is far more dangerous: it becomes chronic in approximately 70 to 90% of cases, and it is this chronic form that leads to rapid liver damage.
HDV spreads through the same routes as HBV: contact with infected blood (needle sharing, needlestick injuries, unsterilized medical equipment), sexual contact, and, less commonly, vertical transmission from mother to child.
Risk Groups
- People who inject drugs (highest risk in high-income countries)
- Recipients of unscreened blood products
- Patients with chronic HBV who have ongoing high-risk exposures
- Communities in endemic regions: Central Africa, the Amazon Basin, Central Asia, Eastern Europe, and Mongolia carry the highest global prevalence
Symptoms
Chronic HDV often progresses silently for years before symptoms appear. When symptoms do occur, they may include: • Persistent fatigue and malaise • Right upper quadrant abdominal discomfort • Jaundice (yellow skin and eyes) • Dark urine and pale stools • Nausea and loss of appetite • Spider angiomas and palmar erythema (signs of advanced liver disease) • Ascites and leg edema in decompensated cirrhosis
Many patients are diagnosed only when liver disease is already advanced. Among a national U.S. cohort of veterans with chronic HBV, nearly 1 in 3 individuals already had advanced liver disease at the time of their first HDV diagnosis, highlighting how frequently the condition is detected too late.
HDV vs. Hepatitis B Alone: Key Differences
| Feature | HBV Alone | HBV/HDV Co-infection |
|---|---|---|
| Global chronic infections | ~257 to 291 million | ~48 to 60 million |
| Rate among HBV carriers | Baseline | ~13% |
| Cirrhosis risk | ~14% in cohort studies | ~40% (OR 3.84 vs. HBV alone) |
| Hepatocellular carcinoma risk | Baseline | ~2x higher |
| Liver transplant risk | Baseline | ~7x higher (HR 7.07) |
| Liver-related mortality risk | Baseline | ~2 to 4x higher (HR 2.05 to 3.78) |
| FDA-approved specific therapy | Yes (multiple) | Yes (bulevirtide, May 2026) |
| Spontaneous clearance (chronic) | Rare | Very rare |
| Disease progression speed | Slow to moderate | Rapid |
Diagnosis
Diagnosing HDV requires a two-step serological approach, and the low rate of reflex testing in clinical practice is a major reason many patients are diagnosed late.
Step 1: Anti-HDV Antibody Screening
The first test is a serum anti-HDV total antibody (IgG/IgM) assay. All individuals who test positive for hepatitis B surface antigen (HBsAg) should be offered this test, per current guidelines from the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL). A positive anti-HDV result confirms exposure but does not distinguish past from active infection.
Step 2: HDV RNA Quantification
HDV RNA by PCR is the confirmatory test for active replication. It is also the primary surrogate endpoint used to assess treatment response. Undetectable HDV RNA (below 50 IU/mL) or a decrease of at least 2 log10 IU/mL from baseline is considered a virologic response.
Liver Disease Staging
Once HDV is confirmed, hepatologists assess the degree of liver damage using
- Transient elastography (FibroScan) to measure liver stiffness in kilopascals, a validated non-invasive marker of fibrosis.
- Liver biopsy when non-invasive tests are inconclusive.
- Alanine aminotransferase (ALT) levels as a marker of hepatocyte inflammation. ALT normalization is the biochemical endpoint used alongside HDV RNA in the MYR301 trial.
- Imaging (ultrasound, CT, MRI) to evaluate for portal hypertension, varices, and hepatocellular carcinoma.
Screening Gap
Despite clear guidelines, HDV testing remains underutilized. In a 2024 U.S. Veterans cohort, only a fraction of HBsAg-positive patients were tested for HDV, and among those tested, 3% were positive for anti-HDV. The approval of a treatment is expected to accelerate adoption of routine reflex testing.
Treatment
Before Hepcludex: The Therapeutic Void
Until May 22, 2026, there was no FDA-approved treatment for chronic HDV. Physicians sometimes used pegylated interferon-alpha (pegIFN-alpha) off-label, but this approach had limited efficacy (response rates of 25 to 30% at best), required 48 to 96 weeks of injections, and caused frequent and often severe side effects including flu-like symptoms, depression, cytopenias, and thyroid dysfunction. Nucleos(t)ide analogs used for HBV (tenofovir, entecavir) suppress HBV DNA but have minimal direct effect on HDV replication.
Hepcludex (Bulevirtide-gmod): Mechanism of Action
Bulevirtide is a first-in-class entry inhibitor. It is a synthetic lipopeptide that mimics the preS1 region of the HBV large surface antigen (L-HBsAg), the domain that binds to the sodium-taurocholate cotransporting polypeptide (NTCP) receptor on hepatocytes. By competitively blocking NTCP, bulevirtide prevents both HBV and HDV from entering liver cells, halting de novo infection of hepatocytes without requiring intracellular viral suppression.
High-quality evidence (Phase 3 RCT): Bulevirtide 8.5 mg once daily by subcutaneous injection.
What the FDA Approved
On May 22, 2026, the FDA granted accelerated approval to Hepcludex (bulevirtide-gmod) 8.5 mg for injection for the treatment of chronic HDV infection in adults without cirrhosis or with compensated cirrhosis. The approval was supported by the Phase 3 MYR301 trial (NCT03852719).
Efficacy Data from MYR301
The MYR301 trial enrolled 150 adults with chronic HDV and compensated liver disease, randomized 1:1:1 to bulevirtide 2 mg daily, bulevirtide 10 mg daily (the dose closest to the approved 8.5 mg), or a 48-week observational control followed by bulevirtide 10 mg for 96 weeks.
Primary endpoint at Week 48 (combined response: undetectable or 2 log10 decline in HDV RNA plus ALT normalization): • Bulevirtide 8.5 mg arm: 48% achieved combined response • Delayed-treatment (control) arm: 2% achieved combined response • Rate difference: 46 percentage points (96% CI: 31 to 61; P less than 0.0001)
Virologic suppression deepened with longer treatment
- Undetectable HDV RNA at Week 48: 20% vs. 0% (control)
- Undetectable HDV RNA at Week 96: 36%
- Undetectable HDV RNA at Week 144: 50%
Post-treatment durability: Final MYR301 data presented at EASL 2025 showed that 36% of patients who achieved undetectable HDV RNA at end of treatment maintained suppression for nearly two years off-therapy. Among patients who had maintained undetectable RNA for at least 96 weeks during treatment, 90% remained undetectable post-treatment.
Safety and Tolerability
Moderate evidence: Bulevirtide was generally well tolerated. The most common adverse events were headache, abdominal pain, fatigue, pruritus, and injection-site reactions.
Boxed Warning: Discontinuation of bulevirtide may result in severe acute exacerbations of both HDV and HBV. Liver function must be monitored closely for at least several months after stopping treatment. Patients should not discontinue bulevirtide without physician guidance.
Hypersensitivity reactions including anaphylaxis have been reported and require standard precautions.
Bile salts: Because bulevirtide blocks the NTCP bile salt transporter, mildly elevated serum bile acids are expected and generally not clinically significant at therapeutic doses.
Regulatory Status
- United States: Hepcludex 8.5 mg - FDA accelerated approval, May 22, 2026 (Gilead Sciences)
- European Union / EEA: Bulevirtide 2 mg - full EMA marketing authorization since July 2023
- Russia, United Kingdom, Australia: Approved at 2 mg
- Note: The FDA had previously rejected the 2 mg dose. The approved U.S. dose of 8.5 mg is higher than the EU dose.
Behind the Research
From Basic Research to the First Approved HDV Drug: ~30 Years in the Making
The story behind bulevirtide is a rare example of a drug born entirely from academic curiosity rather than commercial intent. Its originator is Prof. Dr. Stephan Urban, a virologist and DZIF (German Center for Infection Research) Professor of Translational Virology at Heidelberg University Hospital in Germany.
Stephan Urban and the Heidelberg Laboratory
Roughly 30 years ago, Urban set out with a simple basic-science question: how exactly does hepatitis B virus enter liver cells? During this research he made a pivotal discovery: a fragment of the viral envelope protein binds to a previously unknown receptor on the surface of hepatocytes. That receptor was later identified as NTCP (sodium-taurocholate cotransporting polypeptide), a bile acid transporter. Once Urban and his team understood this mechanism, they synthesized the binding fragment in the laboratory and found it could competitively block the receptor, preventing both HBV and HDV from entering liver cells. This laboratory compound became the molecular foundation of bulevirtide.
The research was conducted at the Department of Molecular Virology, Heidelberg University Hospital, in collaboration with the German Center for Infection Research (DZIF), with structural biology contributions from ETH Zurich.
From Lab to Clinic: The Commercialization Path
To bring the compound from bench to bedside, MYR GmbH, a German biotechnology company, was established to develop bulevirtide commercially. The clinical program advanced through Phase Ib/IIa (2016, first human data published in the Journal of Hepatology), Phase 2 MYR202 (published in The Lancet Infectious Diseases), and ultimately the pivotal Phase 3 MYR301 trial. In late 2020, Gilead Sciences acquired MYR GmbH and took over global development and commercialization of Hepcludex. The European Commission granted conditional approval in 2020, followed by full EMA marketing authorization in July 2023.
Recognition
Prof. Urban's work has been recognized with several major awards
- Baruch S. Blumberg Prize (2023) from the Hepatitis B Foundation, its highest honor
- Chris McGuigan Award for Distinguished Work in Drug Discovery
- Honorary doctorate for outstanding hepatitis research
As Prof. Mathias Munschauer of Heidelberg University Hospital stated at the FDA approval: "Over more than three decades, Prof. Urban has advanced this project with scientific vision, persistence, and leadership, ultimately making a decisive contribution to the development of a therapy for millions of patients."
Multisystem Impact
The Liver Is Not the Only Organ at Risk
In chronic HDV/HBV coinfection, the burden of disease extends beyond hepatocyte inflammation. As liver fibrosis advances unchecked, a cascade of systemic consequences develops:
Portal hypertension: Scar tissue stiffens the liver, raising pressure in the portal vein system. This leads to varices (enlarged veins) in the esophagus and stomach that can rupture and cause life-threatening hemorrhage.
Hepatic encephalopathy: A damaged liver cannot adequately clear ammonia and other neurotoxins from the blood, causing confusion, personality changes, and in severe cases, coma.
Hepatorenal syndrome: Advanced cirrhosis can trigger acute kidney failure due to hemodynamic changes and reduced renal perfusion.
Coagulopathy: The liver synthesizes most clotting factors. In cirrhosis, abnormal bleeding risk increases substantially.
Hepatocellular carcinoma (HCC): HDV infection raises the risk of liver cancer approximately 2-fold compared to HBV monoinfection. In patients with compensated cirrhosis who are anti-HDV positive, the 5-year probability of HCC is estimated at 13%, compared to 4% in HBV-only cirrhotics.
Malnutrition and muscle wasting: Portal hypertension and reduced hepatic synthetic function impair nutrient metabolism and lead to sarcopenia, which independently worsens prognosis.
Quality of life: Studies using patient-reported outcome measures have confirmed that chronic HDV is associated with substantially worse quality of life, fatigue scores, and mental health outcomes compared to HBV monoinfection.
Warning Signs
Red Flags Requiring Urgent Evaluation
The following symptoms in a patient known or suspected to have chronic liver disease warrant same-day or emergency evaluation:
- Vomiting blood or passing black, tarry stools (possible variceal hemorrhage)
- Sudden, severe abdominal pain with distension (spontaneous bacterial peritonitis or acute decompensation)
- Rapid accumulation of abdominal fluid (new-onset ascites)
- Confusion, disorientation, or personality changes (hepatic encephalopathy)
- Yellowing of the eyes or skin that worsens rapidly (acute hepatic decompensation)
- Fever in a patient with known cirrhosis (risk of serious infection)
- Severe fatigue with decreased urine output (hepatorenal syndrome)
Patients who have recently stopped bulevirtide should be monitored especially closely: the boxed warning on Hepcludex explicitly identifies severe acute exacerbation of hepatitis after discontinuation as a potentially life-threatening risk.
When to See a Doctor
Anyone who has ever tested positive for hepatitis B surface antigen (HBsAg) and has not been tested for HDV should ask their physician for an anti-HDV antibody test. This applies even if hepatitis B appears to be well-controlled on antiviral therapy.
See a liver specialist (hepatologist) promptly if
- You test positive for anti-HDV antibodies (follow-up HDV RNA testing is needed)
- You have chronic hepatitis B and develop new or worsening symptoms (fatigue, jaundice, abdominal discomfort)
- You have a history of injection drug use and have not been recently screened for HDV
- You are already on bulevirtide and are considering stopping treatment (do not stop without medical guidance)
- You have been diagnosed with HDV and have not had liver fibrosis staging in the past 12 months
In the United States, the Hepatitis B Foundation's HepDelta Connect program and the Gilead Support Path Program can help patients connect with specialists and navigate treatment access and insurance coverage.
Practical Tips
For Patients Living With HDV
- Get vaccinated: If you have not been vaccinated against hepatitis B, vaccination will prevent HDV (which cannot exist without HBV). If you already have HBV, vaccination will not treat it, but ensuring household contacts are vaccinated protects others.
- Avoid alcohol: Alcohol is independently hepatotoxic and dramatically accelerates liver fibrosis in anyone with underlying liver disease. Even moderate alcohol use is contraindicated in chronic HDV.
- Avoid hepatotoxic medications: Certain pain medications (particularly acetaminophen at high doses), herbal supplements, and over-the-counter products can cause additional liver injury. Discuss all supplements and medications with your hepatologist before taking them.
- Maintain a healthy weight: Non-alcoholic fatty liver disease (metabolic-associated steatohepatitis) and HDV together cause additive liver damage. A Mediterranean-style diet and regular physical activity reduce this risk.
- Screen for liver cancer: Patients with HDV-related cirrhosis should receive liver ultrasound every 6 months plus optional alpha-fetoprotein (AFP) testing for early HCC detection.
- Adhere strictly to bulevirtide if prescribed: Because stopping bulevirtide abruptly can trigger severe hepatitis flares, missing doses or self-discontinuing is dangerous. Discuss any planned interruptions with your doctor well in advance.
- Seek emotional support: Chronic liver disease, especially with limited treatment history, takes a psychological toll. Peer support groups through the Hepatitis B Foundation and patient advocacy organizations can provide community and practical guidance.
FAQ
What is hepatitis delta virus (HDV)?
Hepatitis delta virus (HDV) is a defective RNA virus that can only infect people who already carry hepatitis B virus (HBV). It requires the hepatitis B surface antigen (HBsAg) to assemble and spread. HDV is estimated to infect 48 to 60 million people globally, or approximately 13% of all chronic HBV carriers. There are at least 8 known HDV genotypes, with Genotype 1 being the most widespread and associated with severe disease progression.
Why is HDV considered the most dangerous form of viral hepatitis?
HDV accelerates liver disease far more rapidly than HBV alone. Studies show that patients with HDV/HBV coinfection face a 3.84-fold higher risk of developing cirrhosis compared to those with HBV only. The risk of hepatocellular carcinoma (liver cancer) is approximately 2-fold higher, the risk of needing a liver transplant is 7-fold higher, and liver-related mortality is 2 to 4 times more likely. The cumulative risk of progressing to cirrhosis, liver cancer, liver transplant, or death is estimated at around 70% over the disease course. Compounding the danger, HDV is frequently undiagnosed: nearly 1 in 3 patients in a U.S. veteran cohort already had advanced liver disease by the time they were first tested.
What exactly did the FDA approve on May 22, 2026?
The FDA granted accelerated approval to Hepcludex (bulevirtide-gmod) 8.5 mg injection, manufactured and marketed by Gilead Sciences, as the first and only treatment specifically approved for chronic HDV infection in the United States. The drug was developed originally by the German biotechnology company MYR GmbH, and Gilead Sciences acquired MYR and subsequently advanced bulevirtide through U.S. regulatory review. The approval is under the accelerated approval pathway, meaning it is based on a surrogate endpoint (HDV RNA reduction and ALT normalization) rather than directly demonstrated reduction in cirrhosis or death. Continued approval may depend on results from a confirmatory trial showing definitive clinical benefit.
Who is Hepcludex intended for?
Hepcludex 8.5 mg is indicated for adults with chronic HDV infection who either have no cirrhosis or have compensated cirrhosis (Child-Pugh A). It is not yet approved for patients with decompensated cirrhosis (Child-Pugh B or C). All patients must already be coinfected with HBV, since HDV cannot exist without it. Patients should be on concomitant HBV antiviral therapy (tenofovir or entecavir) as clinically appropriate to manage the underlying hepatitis B infection.
What do we know about bulevirtide's efficacy?
The Phase 3 MYR301 trial is the primary evidence base. At Week 48, 48% of patients receiving bulevirtide 8.5 mg daily achieved the combined response endpoint (undetectable or at least 2 log10 decline in HDV RNA plus ALT normalization), compared to only 2% in the delayed-treatment control group. Undetectable HDV RNA rates increased with longer therapy: 20% at Week 48, 36% at Week 96, and 50% at Week 144. Final post-treatment data (EASL 2025) showed that 36% of patients who cleared the virus during treatment maintained suppression for nearly two years after stopping, and 90% of those who sustained undetectable RNA for at least 96 weeks on treatment remained virus-free off-treatment. High-quality evidence supports virologic and biochemical benefit; evidence on hard clinical outcomes (cirrhosis prevention, death) is not yet established.
What is still not known about Hepcludex?
Several important questions remain unanswered. The FDA approval is under the accelerated pathway, which means that reduction in cirrhosis progression, liver cancer incidence, liver-related death, and need for transplant have not yet been directly demonstrated in clinical trials. The optimal treatment duration is uncertain: the MYR301 trial ran for up to 144 weeks, but whether longer therapy produces proportionally better outcomes or whether a finite treatment course can lead to durable cure in most patients is still being studied. The drug is also not yet approved for patients with decompensated cirrhosis, the group with the highest immediate mortality risk. Long-term safety beyond 144 weeks of use is not yet characterized. Additionally, the impact on HDV genotypes 2 through 8 (less common than Genotype 1) has not been fully characterized in the clinical trial data.
What does this approval mean for patients?
For the approximately 80,000 Americans estimated to live with chronic HDV, this approval is transformational. It is the first time a physician can offer a specifically approved, targeted therapy rather than managing the disease purely by preventing further damage or managing complications. Practically, it means patients with compensated disease now have a treatment option that in clinical trials suppressed the virus in half of treated patients over 144 weeks, with many sustaining suppression after stopping. It is also expected to drive increased screening for HDV among HBV-positive patients, which has historically been extremely low. However, access and cost remain practical considerations: bulevirtide requires daily subcutaneous self-injection, and pricing for rare disease treatments is typically high. Gilead's Support Path Program provides financial assistance and access resources for eligible patients.
Summary
The FDA approval of Hepcludex (bulevirtide-gmod) on May 22, 2026, marks the end of a decades-long therapeutic vacuum in the management of chronic hepatitis delta virus infection. Bulevirtide, a first-in-class entry inhibitor that blocks the NTCP receptor to prevent viral hepatocyte entry, demonstrated a 48-percentage-point advantage over no treatment in the Phase 3 MYR301 trial's primary combined endpoint at Week 48, with virologic suppression continuing to improve through Week 144. The drug is now the first and only FDA-approved treatment for adults with chronic HDV without cirrhosis or with compensated cirrhosis.
Physicians and patients should recognize that the accelerated approval designation means long-term clinical outcomes such as cirrhosis prevention and survival benefit are still under investigation. Close monitoring, strict adherence, and careful management of treatment discontinuation are essential. Patients with chronic HBV who have not yet been tested for HDV should discuss reflex anti-HDV screening with their hepatologist, as timely diagnosis is the prerequisite for timely treatment.
References
- FDA. FDA Approves First Treatment for Chronic Hepatitis Delta Virus (HDV) Infection. May 22, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-chronic-hepatitis-delta-virus-hdv-infection
- Gilead Sciences. FDA Grants Accelerated Approval to Gilead's Hepcludex (bulevirtide-gmod). May 22, 2026. https://www.gilead.com/news/news-details/2026/fda-grants-accelerated-approval-to-gileads-hepcludex-bulevirtide-gmod-the-first-and-only-approved-treatment-for-chronic-hepatitis-delta-virus-hdv
- Hepatitis B Foundation. FDA Approves First-Ever Treatment for Hepatitis Delta. May 26, 2026. https://www.hepb.org/news-and-events/news-2/fda-approves-first-ever-treatment-for-hepatitis-delta-offering-hope-to-80000-americans/
- Pharmacy Times. FDA Approves Bulevirtide-gmod as First-Ever Treatment for Chronic HDV. 2026. https://www.pharmacytimes.com/view/fda-approves-bulevirtide-gmod-as-first-ever-treatment-for-chronic-hepatitis-delta-virus-infection
- HCPLive. Bulevirtide Receives Historic First FDA Approval for Chronic Hepatitis Delta. 2026. https://www.hcplive.com/view/bulevirtide-historic-first-fda-approval-chronic-hepatitis-delta
- Gilead Sciences. Final Data From the Phase 3 MYR301 Study. May 7, 2025. https://www.gilead.com/news/news-details/2025/final-data-from-the-phase-3-myr301-study-demonstrated-longer-treatment-with-bulevirtide-was-associated-with-sustaining-undetectability-after-stopping-treatment
- Rizzetto M, et al. Phase 3 Randomized Trial of Bulevirtide in Chronic Hepatitis D. N Engl J Med. 2023. https://www.nejm.org/doi/full/10.1056/NEJMoa2213429
- Gilead Sciences. Hepcludex Bulevirtide Demonstrates Sustained Efficacy at 96 Weeks. EASL 2023. https://www.gilead.com/news/news-details/2023/hepcludex-bulevirtide-demonstrates-sustained-efficacy-and-safety-profile-in-people-with-chronic-hepatitis-delta-virus-at-96-weeks
- Chen HY, et al. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of HDV Infection. J Infect Dis. 2020;221(10):1677-1687. https://pubmed.ncbi.nlm.nih.gov/31778167/
- Gish RG, et al. Association of Hepatitis Delta Virus With Liver Morbidity and Mortality: A Systematic Literature Review and Meta-Analysis. Hepatology. 2024;79:1129-1140. https://pubmed.ncbi.nlm.nih.gov/37870278/
- Hepatitis B Foundation. Facts and Figures: Hepatitis Delta. https://www.hepb.org/research-and-programs/hepdeltaconnect/factsandfigures/
- Wong RJ, et al. High Prevalence of Cirrhosis or HCC at Hepatitis Delta Infection Diagnosis Reflects Alarming Delays in Testing. PubMed. 2025. https://pubmed.ncbi.nlm.nih.gov/40944453/
- Manesis EK, et al. Influence of HDV Infection on Morbidity and Mortality in Compensated Cirrhosis Type B. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC1727859/
Key Takeaways
- HDV is a defective RNA virus that can only infect people already carrying hepatitis B virus (HBV).
- Approximately 48 to 60 million people worldwide have chronic HDV, representing roughly 13% of all HBV carriers.
- HDV/HBV coinfection carries a 3.84-fold higher cirrhosis risk and 2 to 7-fold higher risks of liver cancer, transplant, and death compared to HBV alone.
- On May 22, 2026, the FDA approved Hepcludex (bulevirtide-gmod) 8.5 mg as the first and only treatment specifically for chronic HDV in the United States.
- Bulevirtide works by blocking the NTCP receptor, preventing both HBV and HDV from entering liver cells.
- In the Phase 3 MYR301 trial, 48% of patients achieved combined virologic-biochemical response at Week 48 vs. 2% with no treatment.
- Virologic suppression (undetectable HDV RNA) reached 50% of patients by Week 144 of treatment.
- The FDA approval is under the accelerated pathway: direct clinical benefit (prevention of cirrhosis, death) has not yet been established.
- A boxed warning highlights the risk of severe acute hepatitis exacerbation if bulevirtide is abruptly discontinued.
- All adults with chronic HBV who have not been screened for HDV should discuss anti-HDV antibody testing with their physician.
Medical Disclaimer
This article is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified physician or hepatologist for any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay seeking it because of something you have read in this article. If you are experiencing a medical emergency, call 911 (US), 112 (EU), or your local emergency services immediately. The information in this article was current as of the publication date but medical guidelines and drug approvals evolve rapidly; verify all clinical information with current guidelines and your healthcare provider.
References
- FDA. FDA Approves First Treatment for Chronic Hepatitis Delta Virus (HDV) Infection. May 22, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-chronic-hepatitis-delta-virus-hdv-infection
- Gilead Sciences. FDA Grants Accelerated Approval to Gilead's Hepcludex (bulevirtide-gmod). BusinessWire. May 22, 2026. https://www.businesswire.com/news/home/20260522569258/en/FDA-Grants-Accelerated-Approval-to-Gileads-Hepcludex-bulevirtide-gmod-the-First-and-Only-Approved-Treatment-for-Chronic-Hepatitis-Delta-Virus-HDV
- Hepatitis B Foundation. FDA Approves First-Ever Treatment for Hepatitis Delta, Offering Hope to 80,000 Americans. May 26, 2026. https://www.hepb.org/news-and-events/news-2/fda-approves-first-ever-treatment-for-hepatitis-delta-offering-hope-to-80000-americans/
- Pharmacy Times. FDA Approves Bulevirtide-gmod as First-Ever Treatment for Chronic HDV. 2026. https://www.pharmacytimes.com/view/fda-approves-bulevirtide-gmod-as-first-ever-treatment-for-chronic-hepatitis-delta-virus-infection
- Rizzetto M, et al. A Phase 3, Randomized Trial of Bulevirtide in Chronic Hepatitis D. N Engl J Med. 2023. https://www.nejm.org/doi/full/10.1056/NEJMoa2213429
- Gilead Sciences. Final Data From the Phase 3 MYR301 Study. EASL 2025. May 7, 2025. https://www.gilead.com/news/news-details/2025/final-data-from-the-phase-3-myr301-study-demonstrated-longer-treatment-with-bulevirtide-was-associated-with-sustaining-undetectability-after-stopping-treatment
- Gilead Sciences. Hepcludex Bulevirtide Demonstrates Sustained Efficacy at 96 Weeks. EASL 2023. https://www.gilead.com/news/news-details/2023/hepcludex-bulevirtide-demonstrates-sustained-efficacy-and-safety-profile-in-people-with-chronic-hepatitis-delta-virus-at-96-weeks
- Chen HY, et al. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of HDV. J Infect Dis. 2020;221(10):1677-1687. https://pubmed.ncbi.nlm.nih.gov/31778167/
- Gish RG, et al. Association of HDV With Liver Morbidity and Mortality: Systematic Review and Meta-Analysis. Hepatology. 2024;79:1129-1140. https://pubmed.ncbi.nlm.nih.gov/37870278/
- Hepatitis B Foundation. Facts and Figures: Hepatitis Delta. https://www.hepb.org/research-and-programs/hepdeltaconnect/factsandfigures/
- Wong RJ, et al. High Prevalence of Cirrhosis or HCC at HDV Diagnosis Reflects Delays in Testing. PubMed. 2025. https://pubmed.ncbi.nlm.nih.gov/40944453/
- HCPLive. Bulevirtide Receives Historic First FDA Approval. 2026. https://www.hcplive.com/view/bulevirtide-historic-first-fda-approval-chronic-hepatitis-delta
- Sciencedirect. Bulevirtide monotherapy in CHD: Efficacy and safety through week 96. J Hepatol. 2024. https://www.sciencedirect.com/science/article/pii/S0168827824003337
Be the first to comment!